

SOAP Note Example SOAP notes are one of the most widely used documentation methods in healthcare. Whether you are a medical student, nurse, physician, therapist, counselor, physical therapist, or another healthcare professional, learning how to write a proper SOAP note is an essential skill.
Good documentation helps improve communication among healthcare providers, supports continuity of care, and creates an accurate legal record of patient encounters. Although SOAP notes follow a structured format, writing them effectively requires critical thinking, attention to detail, and the ability to summarize information clearly.
In this guide, we’ll walk through what a SOAP note is, explain each section in detail, provide a complete SOAP note example, discuss common mistakes, and share practical tips for writing better clinical documentation.
What Is a SOAP Note?
A SOAP note is a standardized method used SOAP Note Example to document patient encounters. The acronym SOAP stands for Subjective, Objective, Assessment, and Plan. Each section focuses on a specific part of the patient’s visit, making documentation organized and easy to review by other healthcare professionals.
The SOAP format has remained popular for decades because it creates consistency in medical records. Instead of writing long narratives that may be difficult to interpret, providers can quickly record relevant information in separate sections. This structure also helps ensure that important clinical details are not overlooked during documentation.
Healthcare professionals across multiple specialties use SOAP notes daily. From hospitals and private clinics to rehabilitation centers, mental health practices, and physical therapy offices, the format has become a universal language for documenting patient care. Regardless of specialty, the goal remains the same: provide accurate, concise, and clinically useful information.
Understanding the Four Parts of a SOAP Note
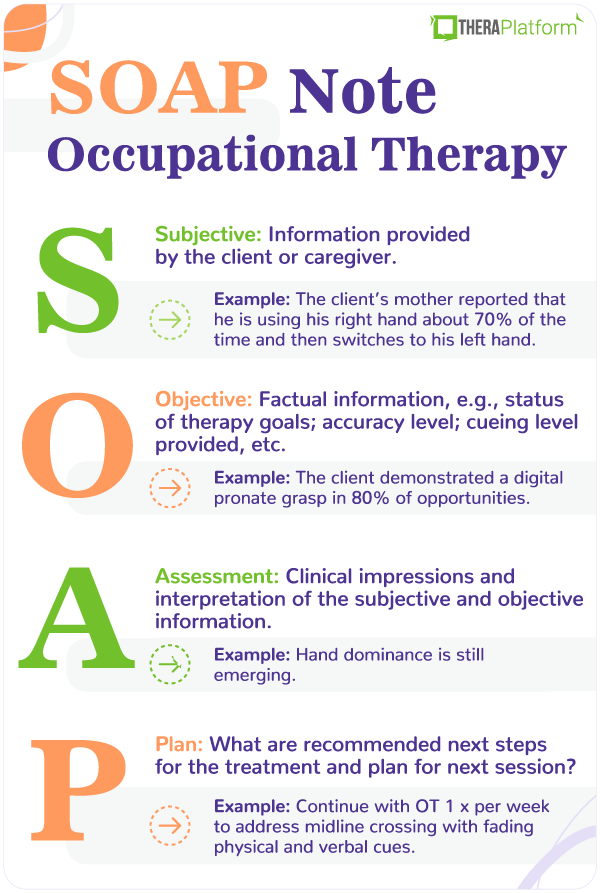
Subjective (S)
The Subjective section includes information directly SOAP Note Example reported by the patient or caregiver. This is where the patient’s own words, symptoms, concerns, and medical history are documented. Providers often record the chief complaint, history of present illness, pain level, medications, allergies, and any relevant lifestyle information.
Because this information comes from the patient, it may not always be measurable or objectively verified. For example, statements such as “I have had a headache for three days” or “My back pain gets worse when I stand” belong in the Subjective section. Recording the patient’s experience accurately helps guide the rest of the clinical evaluation.
A thorough Subjective section also includes details SOAP Note Example about symptom duration, severity, timing, associated symptoms, and factors that improve or worsen the condition. Asking open-ended questions often results in more complete and meaningful documentation.
Objective (O)
The Objective section contains measurable and observable findings collected during the examination. This includes vital signs, physical examination findings, laboratory results, imaging reports, and other diagnostic information.
Unlike the Subjective section, objective information is based SOAP Note Example on facts rather than patient opinions. Blood pressure readings, heart rate, oxygen saturation, body temperature, physical examination findings, and laboratory values all belong here.
Good objective documentation should be clear, organized, and relevant to the patient’s condition. Providers should avoid unnecessary details while ensuring that clinically significant findings are recorded accurately.
Assessment (A)
The Assessment section is the provider’s clinical interpretation of the subjective and objective findings. Here, the clinician evaluates the available information, identifies likely diagnoses, and explains the patient’s current condition.
This section often includes primary diagnoses, differential diagnoses, progress toward treatment goals, or changes in the patient’s condition. The assessment demonstrates clinical reasoning and connects SOAP Note Example the collected information to medical decision-making.
A strong assessment should be concise but thoughtful. Rather than simply repeating previous findings, it should explain what those findings mean and how they influence patient care.
Plan (P)
The Plan outlines the next steps in patient management. This includes medications, diagnostic tests, referrals, patient education, follow-up appointments, lifestyle recommendations, and treatment adjustments.SOAP Note Example
The plan should be practical, specific, and easy to understand. Every recommendation should relate directly to the assessment and support the patient’s overall care goals.
Good planning also includes instructions for monitoring symptoms, recognizing warning signs, and scheduling future evaluations when necessary. Clear planning improves treatment adherence and SOAP Note Example promotes better patient outcomes.
Complete SOAP Note Example
Below is a realistic example demonstrating how the SOAP format works in everyday SOAP Note Example clinical practice.
Patient Name: John Smith
Age: 42 years
Visit Type: Primary Care Follow-up
Subjective
The patient reports experiencing a persistent cough for the past seven days. He describes the cough as dry, occurring throughout the day, and worsening at night. He denies coughing up blood or mucus but reports SOAP Note Example mild throat irritation.
He states that over-the-counter cough medicine has provided minimal relief. He also mentions feeling slightly fatigued but denies fever, chills, chest pain, or shortness of breath. The patient has no recent travel history and reports no known exposure to individuals with respiratory infections. He has a history of seasonal allergies and hypertension controlled with medication.
Objective
Temperature: 98.7°F
Blood Pressure: 128/80 mmHg
Heart Rate: 76 bpm
Respiratory Rate: 16 breaths per minute
Oxygen Saturation: 99% on room air
Physical examination reveals mild erythema of the throat without exudate. SOAP Note Example Lung sounds are clear bilaterally with no wheezing or crackles. No cervical lymphadenopathy is noted. Cardiac examination is normal. The patient appears comfortable and is in no acute distress.
Assessment
Persistent dry cough most consistent with viral upper respiratory infection or post-viral cough. No evidence of bacterial infection or pneumonia at this time. Hypertension remains well controlled on current medication regimen.
Plan
Recommend supportive care, including increased fluid intake, SOAP Note Example warm beverages, and throat lozenges. Continue over-the-counter cough suppressant as needed. Advise rest and monitor symptoms closely. Educate the patient regarding warning signs such as fever, worsening cough, difficulty breathing, or chest pain that would require immediate medical evaluation. Schedule follow-up if symptoms persist beyond two weeks or worsen significantly.
Why SOAP Notes Matter in Clinical Practice
SOAP notes improve communication among healthcare providers SOAP Note Example by organizing patient information into predictable sections. When multiple clinicians care for the same patient, standardized documentation allows everyone to quickly understand the patient’s history, current condition, and treatment plan.
Accurate documentation also contributes to patient safety. Clear records reduce the risk of medication errors, duplicated testing, and missed diagnoses. Providers can easily review previous visits and monitor changes in symptoms over time.
From a legal and administrative perspective, SOAP notes provide evidence of the care delivered during each patient encounter. Insurance companies, auditors, and regulatory agencies often review documentation to verify that appropriate care was provided.
Tips for Writing Better SOAP Notes
Good SOAP notes begin with careful listening. Allow patients to SOAP Note Example describe their concerns without interruption before asking focused follow-up questions. This approach often reveals important details that may influence diagnosis and treatment.
Use clear and professional language throughout the note. Avoid vague SOAP Note Example descriptions or unnecessary abbreviations that may create confusion for other healthcare providers. Precision is especially important when documenting medications, diagnoses, and treatment plans.
Keep documentation concise while including all clinically relevant information. Every sentence should contribute meaningful information that supports patient care. Avoid repeating the same information across multiple sections of the note.
Review your documentation before finalizing it. Even experienced clinicians occasionally make spelling errors, omit important findings, or accidentally include contradictory information. A quick review improves both accuracy and professionalism.
Common Mistakes to Avoid
One common mistake is mixing subjective and objective information. Patient statements should remain in the Subjective section, while measurable examination findings belong in the Objective section. Keeping these categories separate improves clarity and organization.
Another frequent error is writing assessments that simply restate examination findings without offering clinical interpretation. The Assessment should explain what the collected information means and identify the most likely diagnosis or clinical impression.
Some providers also create vague treatment plans that lack specific recommendations. Instead of writing “Follow up as needed,” include detailed instructions regarding medications, follow-up timing, diagnostic testing, patient education, and warning signs requiring immediate medical attention.
Finally, avoid documenting information that was not actually observed or discussed during the visit. Accurate documentation protects both patients and healthcare professionals while maintaining the integrity of the medical record.
SOAP Notes in Different Healthcare Specialties
Although the basic SOAP structure remains the same, different healthcare specialties customize documentation to meet their specific needs. Physicians often focus on diagnosis, laboratory findings, medication management, and disease progression.
Nurses may emphasize patient responses to treatment, vital sign trends, education provided, and ongoing monitoring during hospitalization. Their documentation often supports interdisciplinary communication throughout the patient’s stay.
Physical therapists typically document functional limitations, range of motion, muscle strength, gait analysis, therapeutic exercises, and rehabilitation progress. Mental health professionals may focus more heavily on mood, behavior, thought processes, coping strategies, and therapeutic interventions while maintaining the same SOAP framework.
Best Practices for Maintaining High-Quality Documentation
Consistency is one of the most important qualities of excellent clinical documentation. Following the SOAP format during every patient encounter makes documentation more efficient and easier for colleagues to interpret.
Documentation should always be completed as soon as possible after the patient encounter. Waiting several hours or days increases the likelihood of forgetting important clinical details or introducing inaccuracies into the medical record.
Confidentiality must always remain a priority. Healthcare providers should document only relevant medical information and ensure that patient records remain secure in accordance with applicable privacy regulations and organizational policies.
Continuing education also helps clinicians improve documentation skills. Medical documentation standards evolve over time, particularly with the widespread use of electronic health records. Staying informed about best practices supports better patient care and professional development.
Conclusion
Learning how to write an effective SOAP note is an essential skill for every healthcare professional. The SOAP format provides a logical framework for organizing patient information while promoting consistency, communication, and high-quality clinical documentation.
By clearly separating subjective complaints, objective findings, clinical assessment, and treatment planning, providers create records that support safe, efficient, and patient-centered care.
Whether you are a student practicing documentation for the first time or an experienced clinician refining your workflow, mastering the SOAP note format will improve both your documentation skills and your ability to deliver effective healthcare. Using a well-structured SOAP note example as a guide can make the learning process easier while helping you develop confidence in documenting real-world patient encounters accurately and professionally.

{kind=link}